

By Taylor Knopf
Olehonna Lynch started Pembroke Center for Wellness in 2010 because she wanted people in her home community to receive the best mental health care possible.
Lynch, a psychiatric nurse practitioner, said that before she started her practice the residents of Robeson County waited up to three months for an outpatient psychiatric appointment. When people can’t get help for their mental health issues in the community, they often end up in an emergency room in crisis.
Once they are stabilized, those patients return back home to again wait weeks for an outpatient follow-up appointment.

In contrast, Lynch said she can get a new patient in to see her in less than a week.
“It came down to one of those things where if you want it done right, do it yourself,” she said. “So that’s what I ended up doing. I realized there weren’t many options besides working at the hospital.”
Lynch has a background as a family nurse practitioner and later got her post-master’s certification in psychiatry because she said there was such a “huge need.” Lynch is the owner of her practice where she sees 80 to 100 patients a week and employees an individual and family therapist.
But her practice is tied to a psychiatrist who acts as her “supervisor.”
A North Carolina law passed in the 1970s requires advanced nurse practitioners to have a “collaborative agreement” with an overseeing physician. Essentially, Lynch pays $500 per month for that psychiatrist’s signature twice a year. The supervising physician doesn’t need to approve any treatment decisions or medications for Lynch’s patients. The physician doesn’t even need to be in the same building, or the same city or even the same county.
“I try to utilize her expertise more so that it’s not just a signature,” Lynch said. “If I have a difficult case, I will set up an appointment for my patient to meet with her for a second opinion. So I try to get more out of the collaborative agreement than just a signature and exchange of money.”
Lynch’s supervising psychiatrist works for Veterans Affairs at the local hospital and is planning to retire soon. When she stops practicing, the only psychiatrist in Robeson County — a county with 130,000 people — will be gone.
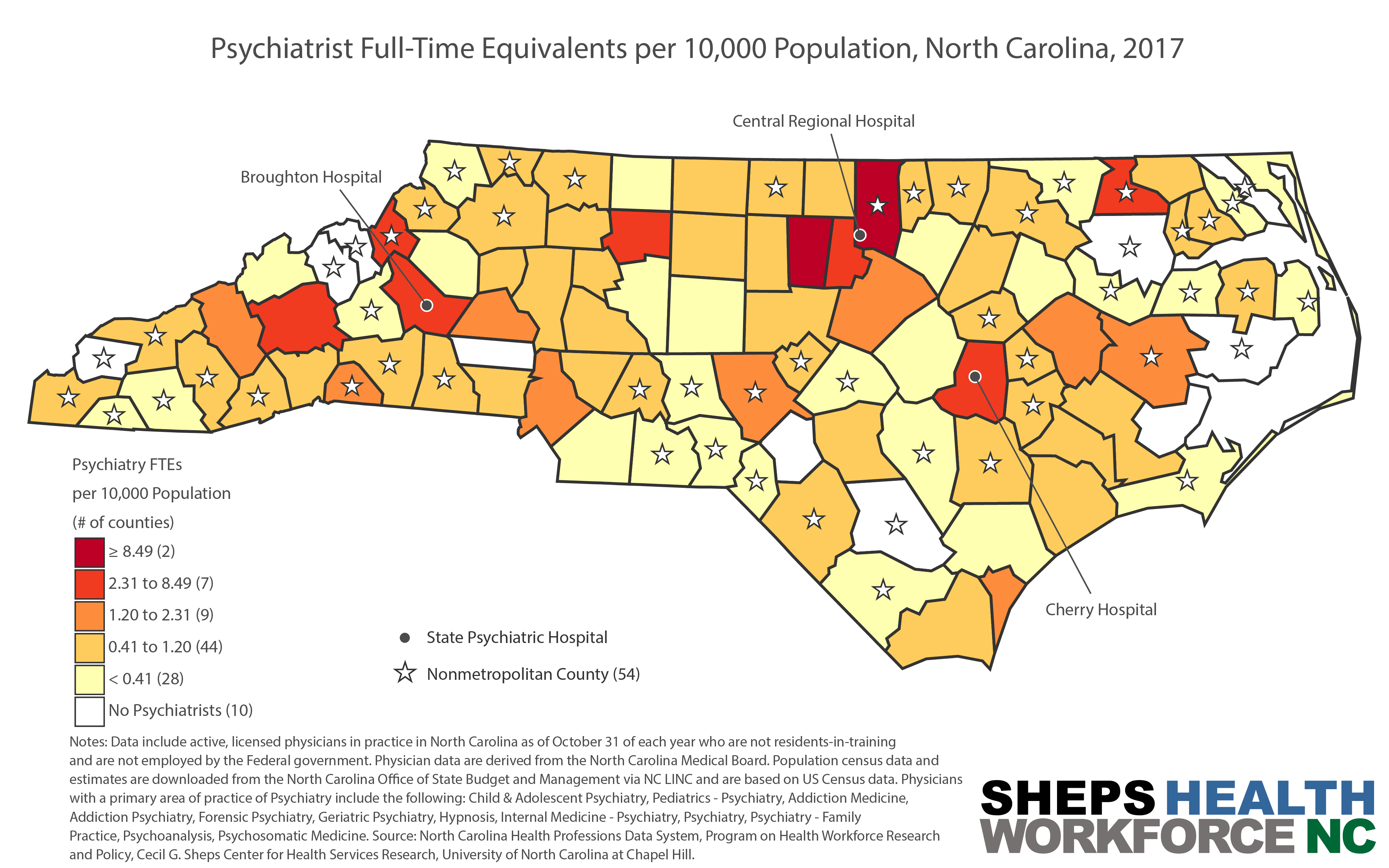
Unfortunately, this is not uncommon in North Carolina. In 2017, the Sheps Center for Health Services Research at the University of North Carolina found that 10 counties have no psychiatrists and 28 counties have less than the equivalent of one full-time psychiatrist per 10,000 people.

The retirement of Lynch’s collaborating psychiatrist also puts Lynch’s practice in jeopardy. Unless the law changes this legislative session, Lynch must have a supervisor to continue running her practice.
The SAVE Act
A bipartisan group of lawmakers has been trying for several years to pass a bill called the SAVE Act to remove that collaborative agreement requirement and allow advanced nurse practitioners to practice in North Carolina with more autonomy.
If the SAVE Act passes, Lynch said she will continue to collaborate with mental health professionals as needed. She said as it is, she consults other medical specialists regularly. Lynch said other advanced nurse practitioners contact her interested in starting their own practices, wanting to learn more about how to do it.
But the collaborative agreement requirement does deter some from moving forward, she said.
Related stories:
Nursing students ready to go to rural NC, but need more autonomy
Advanced practice nurses press legislature for autonomy from MD supervision
“We’re just trying to do the job we are trained to do with the least restrictions possible,” Lynch said. “We’re not trying to be physicians. It’s just difficult to practice with one arm tied behind your back.”
SAVE Act sponsor Sen. Ralph Hise (R-Spruce Pine) said he pushes for the bill every year because the number of health providers in rural western North Carolina continues to decline and his constituents need access to care.
“We tend to put so many barriers from a policy standpoint, to make sure that [advanced nurse practitioners] can’t practice,” Hise said last week during a press conference announcing the filing of the SAVE Act (Senate Bill 249). “The end result is simply that people do not get the health care they need, particularly in preventative services.”

Advanced nurse practitioners are more likely than physicians to practice in a rural area, and North Carolina data shows that nurses who train locally are more likely to practice in a rural area than physicians.
For years, some physicians and their professional societies have opposed this legislation. In the wake of the pandemic, state lawmakers said this year could be different.
“COVID put the spotlight on gaps in our modern health care system, including overcrowded emergency rooms and lack of access,” said Rep. Donna White (R-Clayton), a registered nurse, during the press conference in support of the SAVE Act.
The Save Act will address access but also move toward health equality for marginalized communities, said Rep. Carla Cunningham (D-Charlotte), who is also trained as a nurse.
“You can’t offer coverage to more people if you don’t have the workforce in place to deliver that care,” she said during the press conference.
Hise is more hopeful the bill will pass this time because there have been even more conversations about the benefits of the SAVE Act with people from different parts of the health care system.
“I wish anesthesiologists were more involved in that process, they’ve chosen not to,” Hise said. “But particularly among the other areas that are out there, they have been to the table and been working on this process to get us to this place.”
The North Carolina Medical Society has yet to take a stance on the bill this time around.
“We are in the process of reviewing this latest proposal. The NCMS supports public policy that results in the highest quality of medical care and puts patient safety first,” the society’s spokesperson Elaine Ellis wrote in an email to NC Health News.
Healthier patients, cost savings
If lawmakers would have passed the SAVE Act in 2019, North Carolina could have already saved at least $866 million in health care expenses, argued Sen. Joyce Krawiec (R-Kernersville).
“We can cut costs without cutting corners, and that’s what this bill does in a very effective way. Most bills that are introduced in these chambers usually cost a lot of money,” Krawiec said. “This legislation costs the citizens of North Carolina nothing and the benefits will be staggering.”
The North Carolina Nursing Association cited a 2015 study from the Duke University Center for Health Policy and Inequalities Research which concluded that removing barriers such as the physician supervision requirement would save the state “between $433 million and $4.3 billion per year while creating more than 3,800 jobs.”
“This is an opportunity to lessen the impact of physician shortages without compromising quality of health care,” said Sen. Jim Burgin (R-Angier). “Modernizing regulations is an important part of an evolving health care system.”
Rep. Gale Adcock (D-Wake), the only advanced practice registered nurse in the General Assembly, said the health outcomes of advanced nurse practitioners’ patients are “as good and sometimes better” than their physician colleagues.

“We intend to continue to work with our physician colleagues as true colleagues interdependently as all health care providers do,” said Adcock, who has been a practitioner for 34 years. She just retired from a job where she actually was the boss to the physicians who were her supervisors.
The state is in the middle of transitioning the Medicaid program from one where reimbursement comes for every visit, test and procedure to one where providers get paid a lump sum to deliver more value and healthier patients.
Patient outcomes will be one of the key benchmarks for measuring how well providers are doing.
“You’re paying for how healthy your patient is, and that is not just how healthy is your healthiest patient, but how healthy is your sick patient,” Adcock said. “Advanced practice registered nurses bring a lot of bang for the buck. Because we keep people out of the hospital, we keep them in their homes and out of nursing homes.”
They also tend to be less costly to employ than physicians.
Adcock said that 23 other states and the District of Columbia have allowed their advanced nurse practitioners more autonomy, “and their citizens have not suffered from it.” And no state has reversed that decision, she added.
Mental health provider shortage
Dona Francis is a psychiatric nurse practitioner who runs a mental health practice in Sunset Beach where she sees around 100 patients a week. Right now, she has a big dilemma. The 69-year-old wants to retire but cannot find someone to take over her practice. She says the collaborative agreement requirement is a contributing factor.
Francis’ supervising psychiatrist lives in the Charlotte area, and there are no psychiatrists practicing in Brunswick County. Francis is the only mental health provider in her county of 142,000 residents. The closest psychiatrist is in Wilmington, and the wait for an appointment is at least a month, she said. Many of her clients in Sunset Beach are older and do not want to travel that far.
“A lot of people don’t want to have to go an hour away when they’re already dealing with anxiety and depression,” Francis said. “And COVID has added another layer to that. They feel isolated being unable to see their family, children and grandchildren. Anxiety and depression has increased tenfold from where it was a year ago.”
She’s received a lot of new patients during the pandemic and said she gets new referrals every week. Francis said primary care providers don’t feel comfortable treating a psychiatric diagnosis, and they often don’t feel qualified or have time to do talk therapy with a patient.
“They have people for 15 minutes in their office and they’re out,” Francis said. “They don’t have an hour to sit with someone, help them process what’s going on, deal with their grief or help them with coping skills.”
Francis has been actively talking to nursing schools in the state in a quest to find her replacement. But she said graduating psychiatric nurse practitioners struggle to find a collaborating psychiatrist.
As she continues to search, Francis said she feels like she has an “ethical responsibility to stay the course, until I can get someone here.”
![]()

{kind=link}
Outpatient Psychiatric services are one thing. Inpatient services and Midwifery are quite another – especially in the wake of the 2018 “Baby and Company” fiasco (3 babies died for lack of proper physician oversight of midwives in a for-profit/corporate setting).
And, in the end, we’re still talking about “medical scope creep” that will pit APRNS (and PA’s) against primary care physicians for jobs – with BOTH groups of providers being abused by the giant systems – for profit. “The pandemic made us do it” is not a blanket excuse for everything.
After conversations with midwives I have worked with and greatly respect, I believe that Advanced Practice Registered Nurses should be fully licensed in their craft (as opposed to licensed as RNs – and registered under a doctor’s license) so that they may be allowed to practice as autonomously as is safe in any given circumstance. But direct medical supervision and/or collaborative agreements DO need to remain in place. Especially in the Mother-Baby arena.
It seems to me that what needs to be “reformed” (to improve access) is the NATURE of the medical supervision in selected – BUT NOT ALL – circumstances.
I would also respectfully suggest that, post-pandemic, the SAVE Act be expanded to address much-needed reforms to both the Medical and Nursing Practice Acts – that address things like staffing ratios, medical labor/contract standardization, and whistleblower protection. If you do not do this as you expand nursing independence, you are just throwing APRNs into the same toxic corporate soup where physicians are currently floundering. In an e-mail exchange with Representative Adcock this past week, she was completely non-receptive.
How many nurse practitioners can a physician supervise in NC? It is unlimited and has been for some time. “Supervision” has been abused by physicians and nurses. Most nurses are not really supervised and have learned to have a relationship with a number of physicians they can refer to or call and discuss complex patients that they need help with. Advanced Practice nurses are well trained and are often more willing to ask for help than their physician colleagues. They are willing to serve in areas of need and should be independent since they essentially have been for many years. They need to be monitored for use of controlled substances, just like physicians, to prevent abuse of opioids, etc. The “turf” they occupy is often empty as the article says. Collaboration, not supervision with physicians is what is really needed.
This article highlights the need to make these great folks independent practitioners. They can provide and do provide great care but having to tie them to a physician or psychiatrist in this day and time is ridiculous. Let’s give them the credit to their experience and education they deserve. A generation ago we would be calling these folks GPs. The only difference is depending upon their specialty, they have a lot more specialized training than GPs. Thank them for all they do, especially with our marginalized populations.
The difference in training between primary care physicians and APRN’s is about 20,000 hours. That is NOT equivalent. It’s certainly not “more”.
As a Pediatrician, who has served in rural/community settings for a good portion of two decades (as both a “full scope” and inpatient MD), my experience and training seem to be meaningless now – as community hospitals will ALWAYS “go for the cheap” in Mother-Baby care when they can get away with it.
A trend I am seeing now (employed even by the big billion dollar medical centers to staff their outlying hospitals) is to hire 2 or 3 NNP’s – “supervised” by a Neonatologist who lives many miles/cities away and never sets foot in the facility – and is not available for back-up or “rescue”. That’s not “supervision” – any more than cutting an unsupervised midwife loose in a birth center with no doctor available to attend – or plan in place to rescue emergencies (as happened in 2018 with Baby and Company).
I honestly don’t know why any Pediatrician would train an additional 3 years to become a Pediatric Hospitalist (a new specialty) if an ED Physician/Chief-of-Staff can look me in the eye and tell me that I “can be replaced by a nurse” . . . which happened to me in my last job . . . before I was abruptly fired (without cause) two days after blowing the whistle on an unsafe practice environment and deficient care. For the record, that situation is PUBLIC RECORD – as I was vindicated by a CMS investigation (citing the case I reported as “deficient”) – yet not restored after – but you won’t find the newspapers in this state doing any investigative reporting on it. Even China is protecting its medical whistleblowers now. Not NC. I’ve never gotten a warm/hearty “Thank You” from hospitals for fighting to to protect my patients (and nurses) from bad policy – I’ve only gotten my life upended over and over again.
(P.S. I was not “replaced by a nurse”. I was replaced by several part time doctors – which kind of speaks to my call load and the abusive nature of the for-profit setting.)
Without additional reforms to protect the medical/nursing labor workforce, what do you think they would do to an independent nurse?
I am a psych APRN and live and work in Colorado (independent practice state). There is no question that a MD has more training than a APRN. However, APRNs do specialize just like an MD and thus a MD PCP may not be as comfortable as a psych NP in certain scenarios. Also, my background is in trauma/ICU, PACU. I can’t imagine having to pay a doc to call me twice a year and they have never met me and live hours away. Often, that is the case for CRNAs and APRNs, who start their own practice in these restricted states. Its’ simply a pay off.
Collaboration is key amongst any profession or business. Theres over 30 states that allow APRNs full practice and that number is growing…Massachusetts and California just changed their laws to full practice. Why? because it provides quality care and saves tons of money on the state level.
Physician supervision equals money and control if we are being honest here. I have plenty of MD friends I can call and discuss a case with. No problem. No money exchanged. Guess what, they call me for advise as well.
Change is necessary
In regards to OB and midwives. Most of them do work right alongside a MD. Also, I work with some great midwives . If a mama is delivering in an outpatient OB setting then there are known risks the mom is taking. When delivering in a hospital setting…95% of the time a MD is near by or is on call. supervision vs collaboration. Collaboration definition: the action of working with someone to produce or create something.
Let’s collaborate here folks.
Be well
As a matter of context, there are FOUR types of APRNs – Nurse Practitioners, Clinical Nurse Specialists, Certified Nurse Anesthetists and Certified Nurse Midwives.
Some, by virtue of what they do and where they do it, actually require more direct medical supervision than others. Indeed, in light of the Baby & Company fiasco back in 2018 (a situation I would categorize as “outpatient), and the multiple cases of children dying in dental chairs, I would respectfully suggest that some medical supervision needs to be tightened.
When you’re on the wrong end of even one of the babies delivered without medical supervision . . . even one time . . . it makes an impression. When you received the dead child in the ED (from the dental chair) . . . it makes an impression. ALL the studies the politicians like to plug go OUT the window.
We are NOT doing right by Pediatrics in this state right now – even with the supervision. We are building medical schools to produce doctors that we don’t have enough residency programs to train.
If anyone thinks that doctors “control” medicine in 2021, I have bridge in Brooklyn to sell you.
This IS about money and power and control – as it continues the steady devaluation of the physician in the collaborative team approach to medical care. Corporate interests are driving the current push for APRN “independence” to “replace” physicians and “save” money – so the multi-million-dollar CEOs can make their bonuses.
I ask you. Were those CEO’s ready for the pandemic? Or did the taxpayer have to collaborate to bail them out?
When one is a doctor and told to her face (by another, more powerful doctor) that she can be “replaced by a nurse” . . . or when it actually happens (as it has happened to me – as recently as yesterday) . . . it kind of sours one on the kind of “collaboration” endorsed here.
I’ve been on the wrong end of the evil/malice-soaked things those CEOs can do to doctors (for simple advocacy) on more than one occasion (they are NEVER held accountable). What do you think would happen to a nurse?
Once primary care doctors are pitted against nurse for the same jobs (North Carolina is not Colorado), I sincerely doubt it will help “collaboration” – which right now, appears to be a political buzz word that translates with “going along to get along” (with corporate).
By all means, be well.